Field note
After having a baby, I started noticing something about sleep that I had never really thought about before.
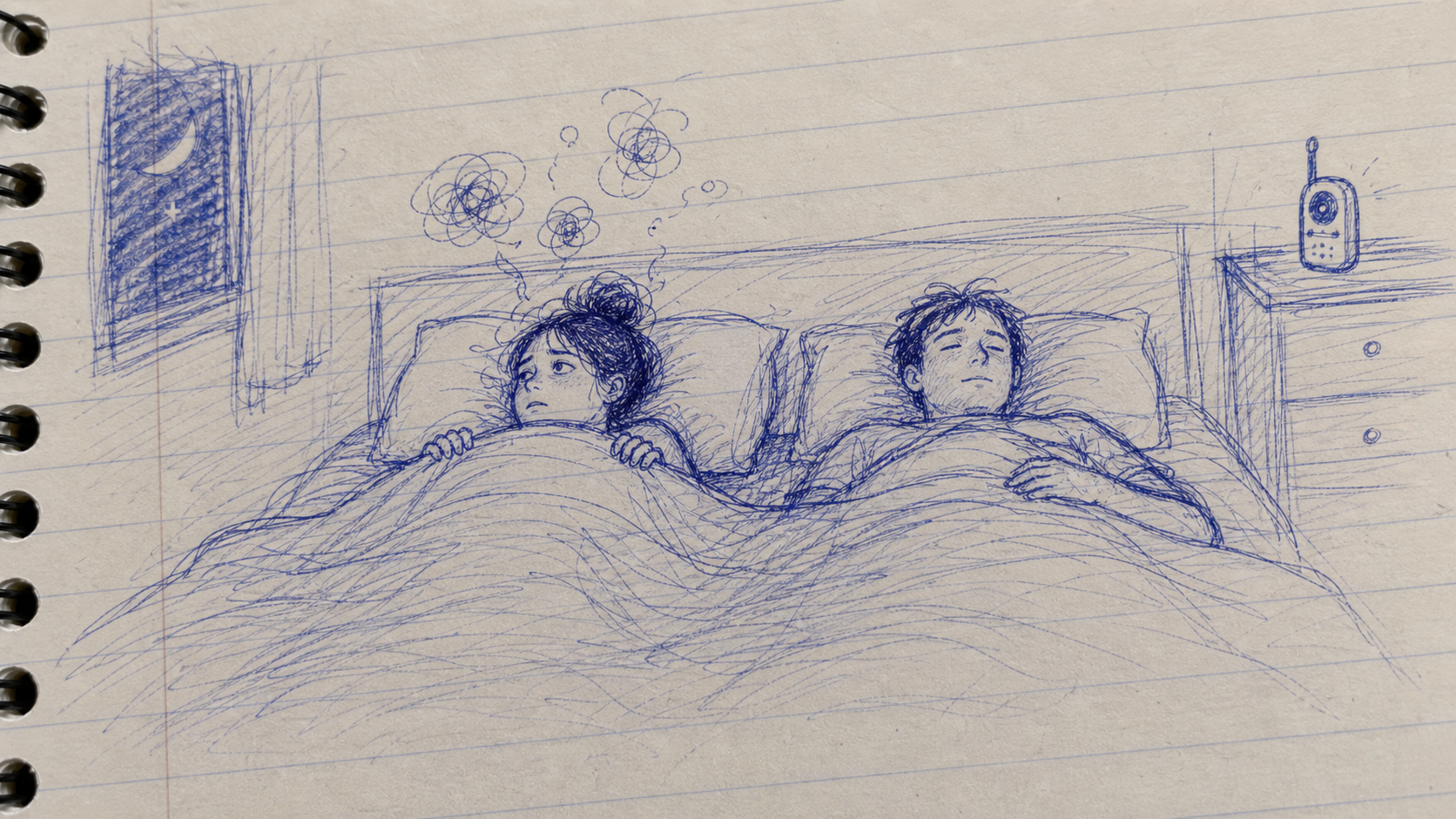
My wife and I were living in the same house, with the same baby, the same random wakeups, and the same broken nights. But we reacted to those nights very differently.
For my wife, one bad night often carried fear into the next one. If she slept badly, bedtime the next day already felt threatening. She would worry that she would not sleep again, that tomorrow would be ruined, that this was becoming her new normal.
I understood why. When you are exhausted and you know the baby might wake up again, bedtime can stop feeling like rest. It can start feeling unsafe.
For me, bad nights were still bad. I would be tired, less sharp, and more irritable the next day. But most of the time I did not treat one bad night as proof that my sleep was broken. I could usually think: that was a bad night. And leave it there.
The difference was not discipline. It was meaning. The same kind of broken night meant something different to each of us.
That made me wonder if, for some people, the thing that hurts most is not only the bad night itself. It is the fear that comes after it.
A bad night can come from anywhere: a baby waking up, stress, caffeine, noise, travel, work, illness, or just bad luck.
But the next night is different. Now you are watching yourself.
Am I sleepy yet? Why am I still awake? What if this happens again? What if this is my life now?
Once that starts, sleep is no longer just sleep. It becomes something you are trying to perform.
A bad night is not automatically a reset. Sometimes it is just a bad night.
Reader notes
I started seeing the same pattern in public sleep conversations. Different situations, but the same shape: the night becomes a test, and fear of failing the test becomes part of the problem.
Reader language
“the second I actually need good sleep”
This was from someone asking why sleep gets worse before important days. The line matters because it shows how quickly sleep can become a performance. The night itself may be ordinary, but the meaning changes: tomorrow matters, so sleep has to work.
That is often when monitoring starts. Every sound, thought, and awake minute gets treated as evidence. The body may be tired, but the mind is checking whether the night is going correctly.
Reader language
“checking if I’m sleepy yet”
This is the loop in its smallest form. The moment you ask whether sleep is arriving, part of the brain is already awake enough to measure it.
That does not mean breathing, relaxation, or other wind-down habits are useless. It means they can change shape. If breathing becomes a trick to force sleep, it becomes another test. If it becomes a signal that the day is over, it can lower the pressure.
Reader friction
“But what do you do when you have dogs?”
This came up in a discussion about CBT-I advice to get out of bed when awake. The question is useful because it pulls sleep advice back into real life. A rule can sound clean on paper and become messy in a house with a partner, pets, noise, and limited space.
The point is not to obey a rule perfectly. The point is to lower the fight around being awake. If getting up turns the whole house on, the “solution” may become part of the problem.
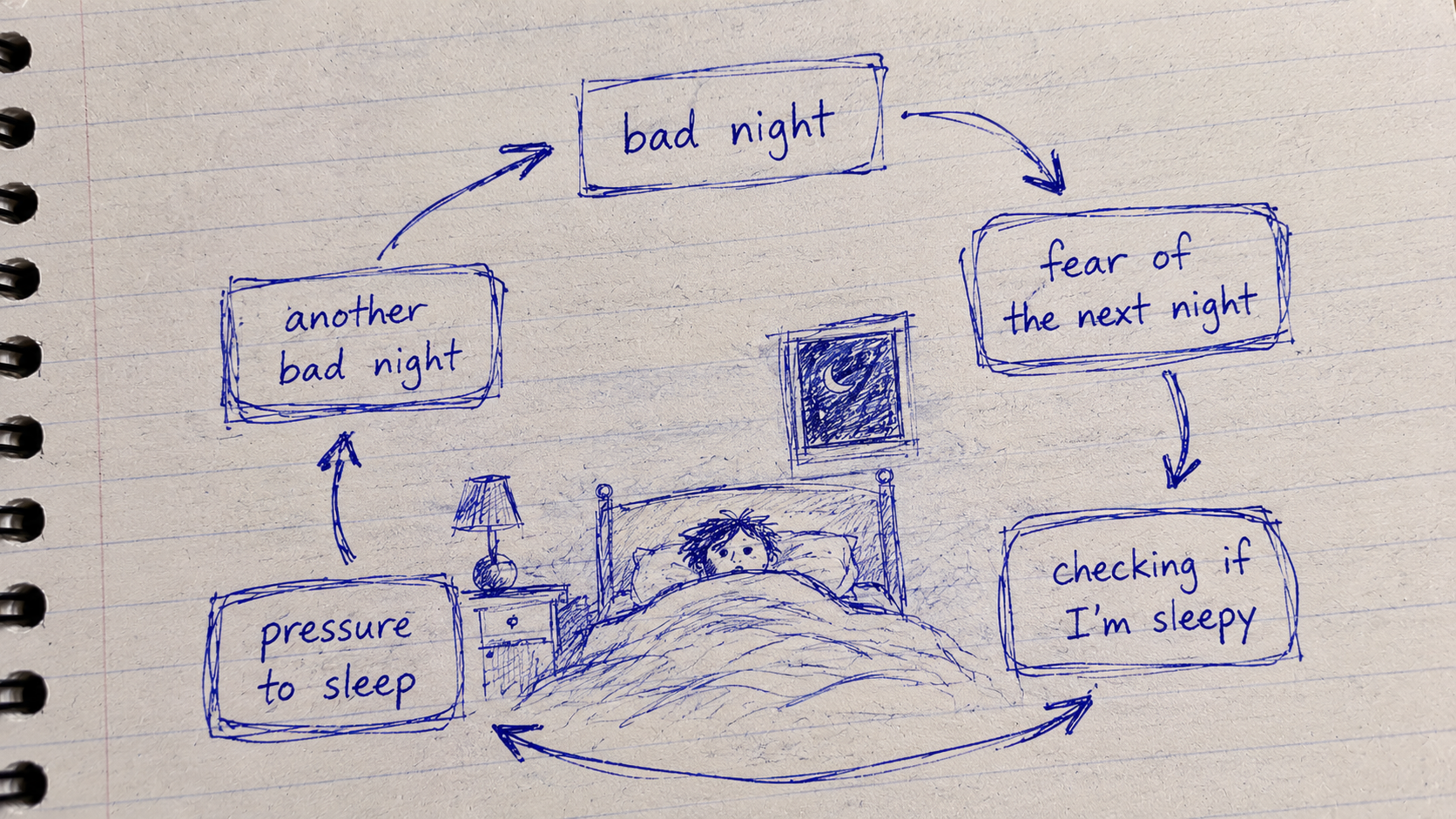
The loop
The loop is simple enough to draw on paper:
bad night → fear of the next night → checking if I am sleepy → pressure to sleep → another bad night.
The first bad night is often specific. Caffeine too late. A stressful interview. A baby waking. A noisy room. A bad shift schedule.
The second problem is more abstract: fear.
Not just “I did not sleep.” More like: what if this happens again? What if I cannot function tomorrow? What if I have insomnia now? What if this becomes my life?
That second fear can be heavier than the original bad night.
Science boundary
I am not saying insomnia is “just anxiety.” It is not. Sleep problems can have many causes, and some need medical help.
The narrower point is that fear of not sleeping can become one of the things that keeps the problem going.
That is close to how classic insomnia models often frame it. The first trigger may be stress, illness, schedule disruption, parenting, or something else. But the factors that keep insomnia alive can include learned associations, monitoring, safety behaviors, worry, and pressure around sleep.
In other words, the first bad night may be caused by life. The second problem may be the meaning we attach to it.
Recovery night
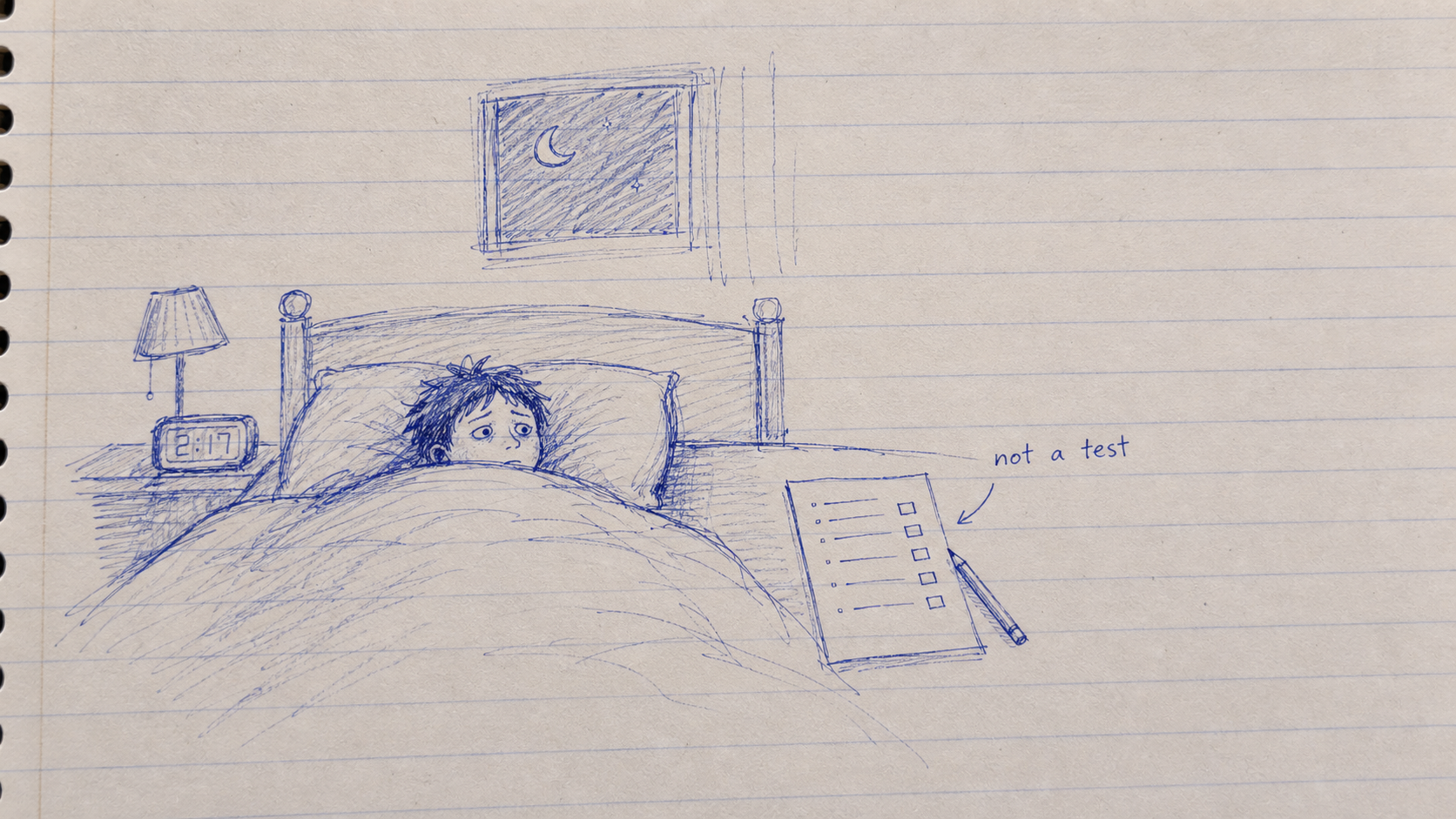
After a bad night, the next night easily becomes an exam.
You lie down and silently ask: am I fixed yet? Am I sleepy enough? Is this going to happen again?
That kind of checking keeps the night important.
The phrase I keep coming back to is: a boring recovery night, not a test.
Not a perfect night. Not proof that everything is solved. Just a low-pressure chance to recover.
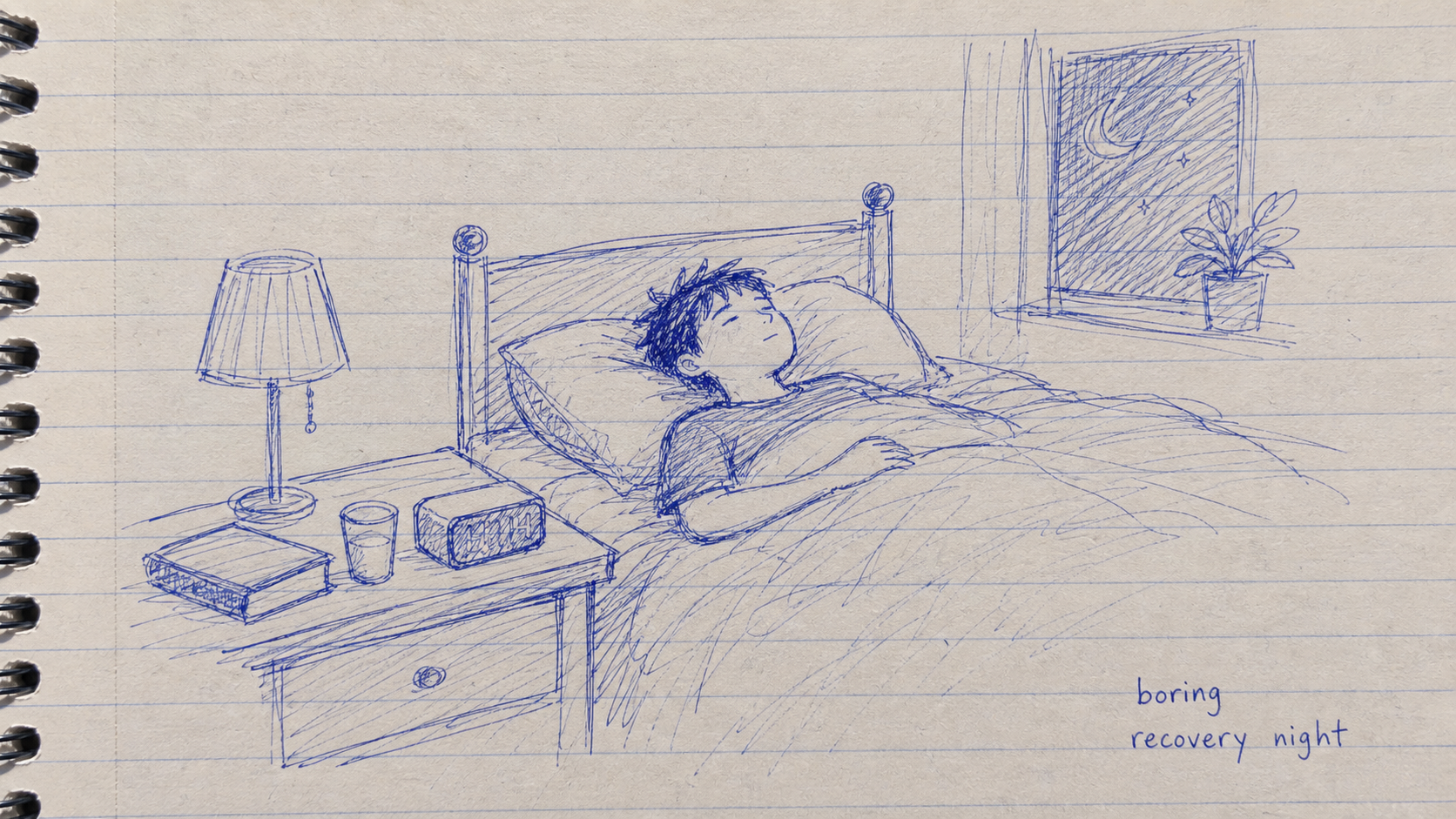
Low expectations. Less checking. Less trying to prove you are fixed.
Just another normal chance for the body to wind down.
Sometimes the work is not to guarantee a good night. It is to stop one bad night from becoming a prophecy.
References and anchors
- Harvey, A. G. (2002). A cognitive model of insomnia. Behaviour Research and Therapy, 40(8), 869-893. doi:10.1016/S0005-7967(01)00061-4.
- Spielman, A. J., Caruso, L. S., & Glovinsky, P. B. (1987). A behavioral perspective on insomnia treatment. Psychiatric Clinics of North America, 10(4), 541-553.
- Edinger, J. D. et al. (2021). Behavioral and psychological treatments for chronic insomnia disorder in adults: an American Academy of Sleep Medicine clinical practice guideline. Journal of Clinical Sleep Medicine, 17(2), 255-262. doi:10.5664/jcsm.8986.